As shown below, total body water (TBW) can be divided into two major compartments: intracellular and extracellular, the latter of which contains both the interstitial and intravascular spaces.
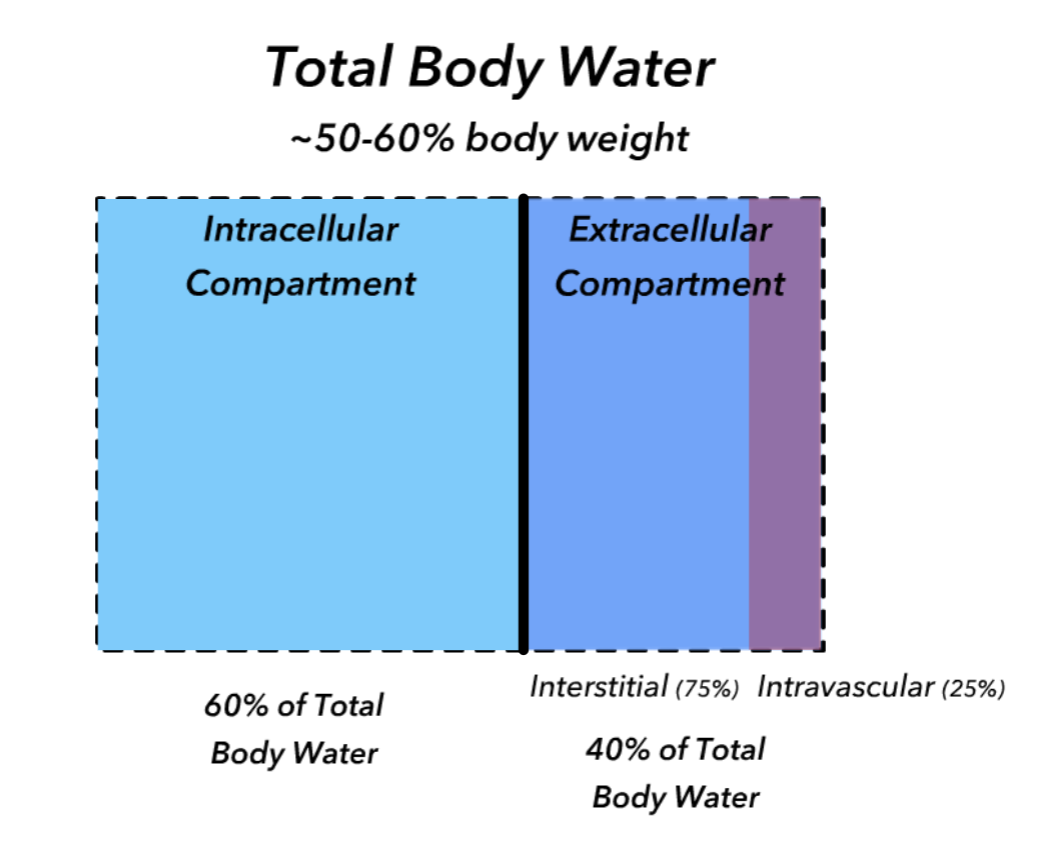
While sodium and potasssium are capable of diffusing across cellular membranes, the sodium-potassium ATPase pumps within the cellular membranes maintain a gradient where sodium is primarily extracellular and potassium is primarily intracellular (left). In contrast, urea is an example of a solute that can freely distribute between fluid compartments (right).
While any dissolved solute may contribute to osmolarity (moles of solute/L), only solutes that respect the intra- and extra-cellular compartment boundaries contribute to "tonicity" by creating an osmotic gradient and cause the distribution of water witihn these compartmenets to shift. Use the
Since fluid shifts between the intra- and extra-cellular compartments can have clinical consequences, tonicity (or effective osmolarity) must be distinguished from total osmolarity, as shown in the equations below. NOTE: the correction factors for glucose and BUN are necessary to convert the units into mmol/L.
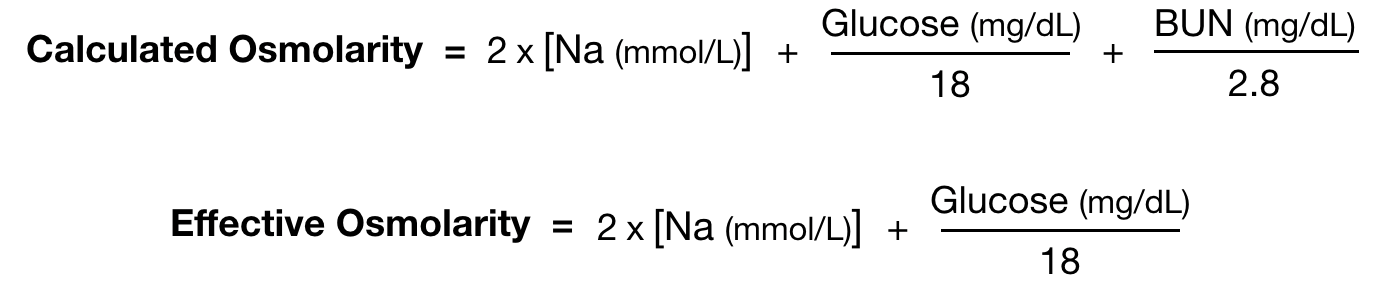
Although excess water can expand volume and excess solute can raise osmolality, we think of effective osmolality (~2 x Na) in terms of water balance we think of and total solute in terms of volume status becauase tonicity is regulated by water homeostasis (via mechanaisms such as thirst and anti-diuretic hormone activity) and the total solute balance is regulated by extracellular volume homeostasis (such as natriuretic peptide activity or RAAS).
Recall that a solute diuresis may contribute to loss of free water if the solute is not an effective osmole, such as in the case of urea.
Calculating electrolyte free water clearance (EFWC) takes into account only effective osmoles to determine how much free water will be lost in the urine. EFWR is the opposite in the context of concentrated urine--how much free water is reabsorbed. See concepts and equations:
Did the EFWC Change after ddAVP was given?
EFWC = UVol x [1 - (UNa + UK)/SNa)]
Did the total daily osmolar output for sodium change?
This simulation assumes that plasma osmolarity is 2x serum sodium and that TBW is 0.6 x weight.
Click this link to view this simulation with additional parameters that are hidden in the view below.
This simulation should NOT be used as a clinical tool.
Not optimized for mobile browsers.